8606 0
Protein
In the process of glomerular filtration, there is almost a wasteless liquid, however, through the filter membrane, nevertheless penetrates the nevertheless number of different proteins. They are absorbed by cells of the proximal tubules; The excretion of the protein in the norm does not exceed 20-75 mg / day, although in some pathological states of proteinuria can reach 50 g / day. The protein reabsorption occurs with a process called pinocytosis.
An increase in the excretion of protein kidney can be due to an increase in the filtering of the protein in the glomers greater than the ability of the tubules to its reabsorption, and the inverse absorption of proteins. There are separate reabsorption systems of various proteins, since TM is detected for hemoglobin, albumin. The proteinuria in the clinic can be detected not only with pathological, but also under a number of physiological states - a large physical activity (marching albuminuria), the transition to the vertical position (orthostatic albuminuria), an increase in venous pressure, etc.
Sodium and chlorine
Sodium and chlorine ions are dominated in extracellular fluid; They determine the osmotic concentration of blood plasma, the regulation of the volume of extracellular fluid depends on their removal or retention of the kidney. Since the composition of ultrafiltrate is very close to extracellular fluid, in the primary urine, the sodium and chlorine ions in the largest quantity are contained, the reabsorption of which in molar expression exceeds the inverse absorption of all other filtered substances combined.
The reabsorption of sodium and chlorine in the distal nephron segment and collecting tubes ensures participation in osmotic homeostasis. It is equally important that the sodium transport system is associated with the transmembrane transfer of a large group of organic and inorganic substances. In recent years, the ideas about the mechanisms, the transport of ions of the nephron cells [Lebedev A. A., 1972 were significantly changed; Naspin Yu. V., 1972; Vogel N., Ullrich K., 1978]. If only sodium transport was considered active, then the ability of cells of one of the nephron departments to the active transport of chlorine ions is currently convincingly demonstrated; . The ideas about the mechanism of reabsorption of fluid in the proximal tubule changed. Below are summarized modern data on sodium reabsorption and chlorine in renal tubules and regulating this process.
In the proximal segment of the nephron, which includes a convulsion and direct channel, about 2/3 of the sodium and water is reabsorbing, but the sodium concentration in the tubular fluid remains the same as in the blood plasma. The peculiarity of proximal reabsorption is that sodium and other reabsorbable substances are absorbed with osmotically equivalent volume of water and the contents of the tubule always remains isooosotic blood plasma. This is due to the high permeability to water the walls of the proximal tube.
Cells of this tube actively reabsorb sodium. In the initial departments of the Canalz, the main anion, accompanying sodium, is bicarbonate; The wall of this piece of nephron for chlorides is less permeable, which leads to a gradual increase in chloride concentration, which increases by 1.4 times compared with blood plasma. In the initial parts of the proximal tubule, glucose, amino acids and some other organic components of ultrafiltrate are intensively reabsorbed. Thus, to the finite parts of the proximal convulsion channel, the composition of osmotic fluid varies significantly - the main mass of bicarbonate is absorbed from it, many organic substances, but becomes higher than the concentration of chlorides (Fig. 1).
It turned out that intercellular contacts in this part of the channel high-dimensional for chlorides. Since their concentration in the lumen is higher than in the near-channel fluid and blood, they are passively reabonored from the tubule, fascinating sodium and water. The reabsorption of sodium and chlorides continues in the direct section of the proximal tubule. In this department, both active sodium transport and the passive reabsorption of chlorides and the movement of the sodium part along with them for intercellular gaps, well permeable for chlorides, occur.
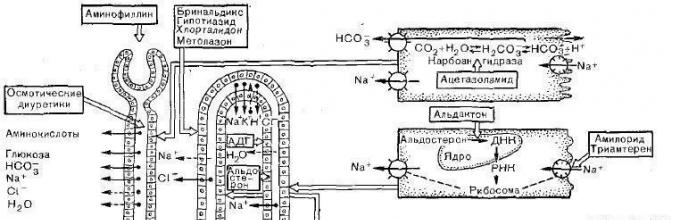
Fig. 1. Localization of reabsorption and secretion of electrolytes and non-electrolytees in nephron. The arrow facing the enlightenment of the Canalza - reabsorption of the substance, in the lumen of the Canalza - secretion.
The permeability of the canal wall for ions and water is determined by the properties of not only the cell membranes, but also the zones of the dense compound, where the cells are in contact with each other. Both of these elements differ significantly in different departments of nephron. Through the apical membrane, sodium cells enters a cytoplasm passively by a gradient of the electrochemical potential, since the inner surface of the cell is electronegative with respect to the tubular fluid.
Next, sodium moves along the cytoplasm to the basal and side parts of the cell, where sodium pumps are located. In these cells, the integral part of the sodium pump is activated by Na + and K + ions dependent on Mg2 + adenosynthosphateza (Na +, K + -TF-AZA). This enzyme, using ATP energy, provides transfer from sodium ion cells and flow into it potassium ions. Inhibitors of this enzyme serve heart glycosides (for example, Wabain, Stroofantin K, etc.) Fully stopping the active reabsorption of sodium cells by cells of the proximal tube.
The zone of cellular contacts is essential in the functional ability of the proximal canal. It occurs through it passive reabsorption of chlorides and the movement of water along the osmotic gradient. It is believed that the absorption rate of fluid in the extracellular gaps is adjusted under the influence of physical forces such as the ratio between the level of hydrostatic pressure in the renal arteries, veins and the ureter, the value of the oncotic pressure in the near-cell capillaries, etc. The permeability of the intercellular gaps is not strictly constant - it can change when A number of physiological conditions. Even a small increase in the osmotic gradient caused by urea, reversibly increases the intercellular permeability in the renal tubules.
In the thin downward department of the loop, the gene does not occur any significant sodium reabsorption and chlorine. A feature of this tube compared to the subtle and thick ascending department of the loop Genla is the high permeability of water. A thin descending loop area The character is low permeability for sodium, but as long as the contrary - high. Having passed on the subtle department of the loop of Genela, the liquid enters the thick-up loop. The wall of this tube always has low water permeability. The feature of the cells of this tube is that the chlorine pump is functioning in them, actively reabsorbing chlorine from the enlightenment of the Canalza, sodium should be passively in a gradient. It is unclear whether the passive sodium passive reabsorption occurs in this channel or the sodium pump is partially functioning.
From a clinical point of view, it is important that the opening of the chlorine pump coincided with the clarification of the mechanism of action of a number of the most effective modern diuretics. It turned out that only with the introduction into the lumen of the thick-rising loop of the loop furosemid and the stacrinic acid completely oppress the reabsorption of chlorine. They bind to the membrane cell elements from the inside of the tube, prevent chlorine intake into the cell, and therefore ineffective when adding to extracellular fluid (Fig. 2). These diuretics come into the magnitude of nephrone when filtering and secretion in the proximal tube, with a stream of urine reach the rising loop of Genela, stop the reabsorption of chlorine and thereby prevent sodium suction here.

Fig. 2. The scheme of regulation of transport of sodium and chlorides in the kidney and the mechanism of action of diuretics [Naspin Yu. V., 1977]. A solid arrow shows active transport, dotted - passive.
The thick ascending department of the loop of Genela goes into the direct part of the distal tube, reaching the Macula Densa region, followed by a distal convulsion canal. This nephron department is also a permeable for water. The leading mechanism for the reabsorption of salts in this tube is a sodium pump that provides sodium reabsorption against a high electrochemical gradient. The peculiarity of the sodium reabsorption in this department is that only only 10% of the sodium filtered and the reabsorption rate can be reduced here than in the proximal channel, but a larger concentration gradient is created, sodium concentration and chlorine in the lumen may decrease to 30-40 mmol / l. Unlike sodium, chlorine reabsorption takes place mainly passively.
The binding department connects the distal nephron segment with initial departments of collecting tubes. These tubules used to be considered passive urine conductors to the urinary system are the most important kidney structures, subtly and precisely reacting to the action of hormones and adapting the work of the kidney to the needs of the body. In these tubules, the base of reabsorption is the sodium pump, chlorides are rehabited passively. The wall of the tubules can be not only waterproof, but also high-pressure water in the presence of ADG. It is in this department of the tubules (and not in the distal segment, as believed before) there is an ADG.
Sodium transport in these cells is regulated by aldosterone. The change in the nature of ion transport and thereby the properties of carriers and pumps are reflected on the features of the chemical structure of diuretics, which are effective in this area of \u200b\u200bnephrone. Veroshriron, amyloride, triamtenen act in these tubules. Veroshpiriron reduces sodium reabsorption, competitively reducing the effect of aldosterone. A completely different mechanism of action in amyloride and triamterene. These drugs act only after they fall into the lumen of the nephron. They bind to those chemical components of the apical membrane, which provide sodium input to the cell; Sodium cannot reabsorb and excreted with urine.
Cortical deposits of collecting tubes are moving into departments passing around the kidney cerebral. Their function is characterized by the fact that they are able to actively reabsorbing very small amounts of sodium, but can create a very high concentration gradient. The wall of these tubules is low-permeable for salts, and its water permeability is adjusted by ADG.
Clinical nephrology
ed. EAT. Tareev
The human body and the excretion of the human excretory system is carried out. The work of the human excretory system organs has its own mechanisms for the dismissal mechanisms for filtering, reabsorption and secretion.
Outline system of man
The excretion of the exchange products from the body is carried out which consist of kidneys, ureters, bladder and urethra.
The kidneys are located in the retroperitoneal space in the area of \u200b\u200bthe lumbar department and have a bean-shaped form.

This is a paired organ consisting of cortical and brainstatus, lochanks, and it is covered with a fibrous shell. Lohanka kidney consists of a small and large bowl, and a ureter comes out of it, which delivers urine into the bladder and through the urethra finite urine is removed from the body.
The kidneys are involved in metabolic processes, and their role in ensuring the water balance of the body, maintaining acid-alkaline balances are fundamental to the full existence of a person.
The structure of the kidney is very complex and its structural element is nephron.

It has a complex structure and consists of a proximal channel, the taurus of the nephron, a loop of the genle, the distal channel and a collective tubule, which gives rise to ureters. The reabsorption in the kidneys passes through the tubes of the proximal, distal and loop of Genela.
Reabsorption mechanism
Molecular mechanisms of passing substances in the process of reabsorption is:
- diffusion;
- endocytosis;
- pinocytosis;
- passive transport;
- active transport.
Active and passive transport and the direction of reabsorbable substances for the electrochemical gradient and the presence of a carrier for substances, the operation of cell pumps and other characteristics are particular importance for reabsorption.
Substances are against an electrochemical gradient with considerable energy on its implementation and through special transport systems. The nature of the movement is transcellorular, which is carried out by the transition through the apical membrane and basolateral. Such systems are:
- Primary-active transport, which is carried out by energy from the splitting of ATP. It uses Na +, Ca +, K +, H + ions.
- Secondary-active transport, passes due to the difference in the concentration of sodium ions in the cytoplasm and in the enlightenment of the tubules, and this difference is due to the yield output of sodium ions in the intercellular fluid with the cost of ATP splitting energy. It uses amino acids, glucose.
It takes through gradients: electrochemical, osmotic, concentration, and for its implementation does not require the cost of energy and the formation of the carrier. Substances that use it are cl- ions. The movement of substances is carried out paracellularly. This movement through the cell membrane, which is located between two cells. The characteristic molecular mechanisms are diffusion, the transfer with the solvent.
The reabsorption process of the protein passes inside the cell fluid, and, after splitting it on the amino acids, they enter the intercellular fluid, which is due to the pinocytosis.
Types of reabsorption
Reabsorption is a process passing in the tubules. And substances passing through the tubules have different carriers and mechanisms.

A day in the kidneys is formed from 150 to 170 liters of primary urine, which passes the reabsorption process and returns to the body. Substances having highly dispersed components cannot pass through the tubing membrane and in the reabsorption process enter the blood with other substances.
Proximal reabsorption
In the proximal department of nephron, which is located in the cortical substance of the kidney, reabsorption is passed for glucose, sodium, water, amino acids, vitamins and protein.

The proximal channel is formed by epithelial cells, which have a apical membrane and brush cut, and it is addressed toward the lumen of the renal tubules. The basal membrane forms folds forming a basal labyrinth, and through them the primary urine enters peritubular capillaries. The cells between themselves are connected tightly and form space, which passes throughout the intercellular space of the tube, and it is called the baselateral labyrinth.
Sodium reabsorption has a complex three-stage stage, and it is a carrier for other substances.
Reabsorption of ions, glucose and amino acids in the proximal canal
The main stages of sodium reabsorption:
- Passage through the apical membrane. This is the stage of passive sodium transport, through Na-channels and Na carriers. Sodium ions are in a cage through membrane hydrophilic proteins that form NA channels.
- Admission or passage through the membrane is associated with the Na + exchange to hydrogen, for example, or with the flow of it as a glucose carrier, amino acids.
- Passage through the basal membrane. This is the stage of active transport Na +, through Na + / K + pumps with the help of an ATP enzyme, which, when splitting, highlights energy. Sodium, reabsorbing in the renal tubules, is constantly returning to metabolic processes and its concentration in the cells of the proximal tube - low.
The glucose reabsorption passes through the secondary-active transport and its receipt is facilitated by transferring it through the Na-pump, and it is completely returning to the metabolic processes in the body. Increased glucose concentration does not pass completely reabsorption in the kidneys and stands out with the final urine.

Amino acid reabsorption is similar to glucose, but the complex organization of amino acids requires the participation of special carriers for each amino acid to less than 5-7 additional.
Reabsorption in the loop of Genela
Loop Galen passes through and the reabsorption process in the ascending and downward part of it for water and ions is different.
The filtrate, falling into the descending part of the loop, going down on it, gives water due to a different pressure gradient and is saturated with sodium and chlorine ions. In this part, the water is reabsorbed, and for ions it is impenetrable. The ascending part of the impenetrable water and when passing through it, the primary urine is diluted, while in the descending concentrates.
Distal reabsorption
This nephron department is located in the cortony of the kidney. Its function consists in reabsorption of water, which is assembled with the primary urine and exposes the reabsorption of sodium ions. Distal reabsorption is the breeding of primary urine and the formation of urine finite from the urine filtrate.
By entering distal channels, the primary urine in a volume of 15% after reabsorption in the renal tubules is 1% of the total volume. Assessed after this in a collecting tube, it is diluted, and the final urine is formed.
Neuro-humoral regulation of reabsorption
The reabsorption in the kidneys is regulated by the sympathetic nervous system and hormones of the thyroid gland, hypothalamic-pituitary and androgen.
The reabsorption of sodium, water, glucose increases when the sympathetic and wandering nerves are excited.
The distal tube and collecting tubes are carried out by the reabsorption of water in the kidneys under the influence of antidiuretic hormone or vasopressin, which, with a decrease in water in the body, increases in large quantities, and also increases the permeability of the tubuine walls.
Aldosterone increases the reabsorption of calcium, chlorine and water, as well as atropeptide, which is produced in the right atrium. The oppression of sodium reabsorption in the proximal department of nephrone is under parastrine.
Sodium reabsorption activation goes at the expense of hormones:
- Vasopressin.
- Glucucan.
- Calcitonin.
- Aldosterone.
The oppression of sodium reabsorption goes when the hormones are generated:
- Prostaglandin and Prostaglandin E.
- Atropeptide.
The brain cortex carries out the regulation of urine removal or braking.
The tube reabsorption of water is carried out by a plurality of hormones responsible for the permeability of the membrane of the distal nephron, the regulation of transporting it through the canal holders and much more.
Reabsorption value
The practical application of scientific knowledge about what reabsorption is in medicine made it possible to obtain informational confirmation of the operation of the organism excretory system and look into the internal mechanisms. It takes very complex mechanisms and the impact on it of the environment, genetic deviations. And they do not remain unnoticed when problems arise on their background. In short, health is very important. Watch it for all the processes occurring in the body.
Back in 1842, the German physiologist K. Ludwig assumed that the urine consists of 3-processes. In the 20s of the twentieth century, American physiologist A. Richards confirmed this assumption.
The formation of the final urine is the result of three consecutive processes:
I. In the renal gloms, the initial stage of urinations occurs - cluster, or glomerular ultrafiltration showless fluid from plasma of blood in a kidney glider capsule, resulting in primary urine.
II. Canal reabsorption - The process of reverse absorption of filtered substances and water.
III . Secretion . Cells of some sections of the tubular are transferred from extracellular fluid into the magnesium lumen (secrete) a number of organic and inorganic substances or separated into the lumen of the tubular molecules synthesized in the Channel cell.
I.Glomelar filtration
The formation of urine begins with glomerular filtration, i.e. Transfer fluid from glomerular capillaries in the bowman capsule, while the liquid passes through the glomerular filter.
Filtering membrane. The filtration barrier in the renal caller consists of three layers: endothelium glomerular capillaries, basal membrane and single-row layer of epithelial cells, The lining capsule of Bowman. The first layer, endothelial capillar cells, perforated with a plurality of thumbs ("windows" or "phenetres") (d times 40 - 100 nm). The basal membrane is a geelectric, a cell-free cellular education consisting of glycoproteins and proteoglycans. The cells of the epithelium capsule, which rest on the basement membrane, are called the Name of Podrocytes. Potocytes an unusual osmedy-like structure, as a result of which they have many finger-shaped processes depressed in the basal membrane. Slim-shaped spaces between the palpal proceeds located nearby are aisles for which the filtrate, passing endothelial cells and the basal membrane, penetrates the Bowmanly space (D slots between the pediculas of the noise 24-30 nm)
In the basement membrane there are pores (d Pores 2.9 - 3.7 nm)which limit the passage of shaped blood elements, as well as large molecules more than 5-6 mm (molecules. Weight more than 70000 Yes: molecules that have MM less than 70,000 are filtered: all minerals, organic compounds (with the exception of large-molecular proteins, lipoids)
Therefore, large proteins, such as globulins (mol. Weste, 160,000) and caseins (mol. Weight 100,000) do not come to the filtrate. Albumin of blood plasma (molter of about 70,000) pass into the filtrate in an insignificant amount. In the lumen of the nephron capsule penetrates inulin about 22% of egg albumin, 3% hemoglobin and less than 0.01% serum albumin (in the case of hemolysis) in this way, filtering occurs. The free passage of proteins through the glomerural filter is hampered by negatively charged molecules in the substance of the basal membrane and the liner lying on the surface of the sub-regional, since the overwhelming number of plasma proteins carries almost only negative electrical charges. With a certain form of kidney pathology, when a negative charge disappears on the membranes, becoming "permeable" with respect to proteins.
Permeability of the glomerular filter It is determined by the minimum size of molecules that are capable of filtered and depends on: 1) pore size; 2) charge charge (basal membrane - anion); 3) hemodynamic conditions; 4) the work of the pediculus of the pecisites (they have actomosic yarns) and merzangilation cells.
In its composition, ultrafiltrate is the primary urine isotonic blood plasma. Inorganic salts and low molecular weight organic compounds (urea, urinary acid, glucose, amino acids, creatinine) - freely pass through the glomerular filter and come to the cavity of the Bowman capsule. Basic force ensuring the possibility of ultrafiltration in renal gloms, is the hydrostatic blood pressure in the vessels. Its value is due to the fact that bringing arteriols - more in diameter than that enduring, as well as the fact that the renal arteries depart from the abdominal department of the aorta.
Filtering area in two kidneys is 1.5 m 2 per 100 g of tissue (i.e., it is equal to the surface of the body. - s body of 1.73 m 2). Depends on : 1) the surface area of \u200b\u200bthe capillaries; 2) the amounts of pores (more than in any other organ; their share accounts for up to 30% of the surface of endothelial cells); 3) the number of functioning nephrons.
Effective filter pressure (EFD), on which the speed of glomerular filtration depends, is determined by the difference between the DGC (hydrostatic blood pressure) in the glider capillaries (in person from 60-90 mm. Hg) and hydrostatic pressure of fluid (or ultrafiltrate) or in a glider capsule about 20 mm.rt.st.
EFD \u003d GDK- (CH + GDU)
EFD \u003d 70 mm.rt. - (30 mm.rt.st. + 20 mm.rt.st.) \u003d 20mm.rt.st.
EFD may vary from 20 to 30 mm.T.. Filtration occurs only if the blood pressure in the glomerular capillaries exceeds the amount of the oncotic pressure of proteins in the plasma and fluid pressure in the slurry capsule. With an increase in filtration pressure, diuresis increases, with a decrease - decreases. The blood pressure in the capillaries of the glomers and the blood flow through them is almost not changed, since, with an increase in systemic arterial pressure, the tone of the opposing arteriole increases, and when the systemic pressure decreases, its tone decreases (the effect of witness - beylis).
Factors defining filtration
Renal factors
To-in functioning gloms
The diameter of the bringing and enduring vessels
Pressure filtrate in the capsule
Exposable factors
General functional condition of the circulatory system, to-in circulating blood, the value of blood pressure and blood flow rate
The degree of hydration of the body. Osmotic and oncotic pressure.
Functioning of other urine removal mechanisms (sweat glands )
Number of primary urine - 150-180 l / day. Through the kidneys per day, 1700 liters of blood flows. Speed \u200b\u200bof glomerular filtration 125 ml / min in men and 110ml / min in women. Thus, about 180 liters per day. The average total plasma volume in the human body is approximately 3 liters, which means that the entire plasma is filtered in the kidneys about 60 times a day. The ability of the kidneys to filter such a huge volume of plasma makes it possible to excrete a significant amount of finite products of metabolism and very accurately adjust the elemental composition of the fluids of the body.
II.Canal reabsorption
In kidneys, a person for one day is formed to 170 liters of filtrate, and 1-1,5l finite urine is released, the remaining liquid is absorbed in the tubules. Primary urine isotonic blood plasma (that is, it is a blood plasma without proteins) The reverse absorption of substances in the tubules is to return all the vital substances and in the necessary quantities of primary urine.
Reabsorption volume \u003d ultrafiltrate volume - the volume of finite urine.
Molecular mechanisms involved in the implementation of reabsorption processes are the same as the mechanisms acting during the transfer of molecules through plasma membranes in other parts of the body is diffusion, active and passive transport, endocytosis, etc.
There are two ways for the movement of the reabsorbable substance from the lumen in the interstitial space.
The first is the movement between the cells, i.e. through a dense connection of two adjacent cells - this is a paracellular way . Paracellular reabsorption can be carried out by diffusion or by transferring a substance together with the solvent. The second way of reabsorption - transcellular ("through" cell). In this case, the reabsorbed substance should overcome two plasma membranes on their way from the enlightenment of the station to an interstitial fluid - luminal (or auxiliary) membrane separating the liquid in the enlightement of the channel from the cytoplasm of cells, and the baselateral (or counterfeit) membrane separating the cytoplasm from the interstitial fluid. Translationllular transport Determined by the term active For brevity, although the intersection of at least one of two membranes is carried out by means of a primary or secondary process. If the substance is reabidorized against electrochemical and concentration gradients, the process is called active transport. Distinguish two types of transport - primary-active and secondary-active . Primary-active transport is called in the case when the substance is transferred against an electrochemical gradient due to the energy of cell metabolism. This transport is provided by the energy obtained directly during the splitting of ATP molecules. An example is the transport of Na ions, which occurs with the participation of Na +, K + ATPase using ATP energy. Currently, the following primary transport systems are known: Na +, K + - Atthase; N + -atphase; N +, K + -ATPAZ and CA + ATPase.
Secondary active It is called the transfer of a substance against the concentration gradient, but without the cost of the energy of the cell directly to this process, glucose, amino acids are reabsorbed. From the enlightenment of the station, these organic substances come into the cells of the proximal tubule using a special carrier, which must be attached to the Na + ion. This complex (carrier + organic substance + Na +) contributes to the movement of the substance through the brush cut membrane and its flow inside the cell. The driving force of these substances through the apical plasma membrane is less than the concentration of sodium in the cytoplasm of the cell. The sodium concentration gradient is due to the direct active sodium excretion from the cell into the extracellular fluid using Na +, K + -atphase, localized cells in lateral and basal membranes. NA + CL reabsorption represents the most significant process in terms of volume and energy costs.
Various deposits of renal tubules differ in the ability to absorb substances. Using the analysis of liquids from different parts of the nephron, the composition of the liquid and the peculiarities of the work of all nephron departments were established.
Proximal canal. Reabsorption in the proximal segment - bond (mandatory). In the proximal convulsion canals, most of the components of the primary urine with equivalent amount of water (the volume of primary urine decreases by about 2/3). Amino acids, glucose, vitamins, the required amount of protein, microelements, a significant amount of Na +, K +, Ca +, Mg +, Cl _, Ca +, Ca +, CL _, HCO 2 are completely reabsorbed in the proximal department of nephrone. The proximal channel plays a major role in the return of all these filtered substances into blood using effective reabsorption. The filtered glucose is almost completely rebupping by the cells of the proximal tubule, and in normal one per day with the urine there may be a minor amount (no more than 130 mg). Glucose moves against a gradient from the enlightenment of the station through the luminal membrane to the cytoplasm through the system of the catransports with sodium. This glucose movement is mediated by the participation of the carrier and is secondaryly active transport, since the energy required for the movement of glucose through the luminal membrane is produced due to the sodium movement by its electrochemical gradient, i.e. Through the kittens. This mechanism of machines is so powerful, which allows you to completely absorb all glucose from the enlightenment of the Canalza. After penetration into the glucose cell, the baselateral membrane should overcome, which occurs, which is independent of the sodium participation of the lightweight diffusion, this movement along the gradient is maintained due to the high concentration of glucose accumulating in the cell, due to the activity of the luminal process of the catransport. To provide active transcellular reabsorption, system functions: with the presence of 2 membranes, which are asymmetry with respect to the presence of glucose carriers; Energy is released only when overcoming one membrane, in this case luminal. The decisive factor is that the entire process of glucose reabsorption depends ultimately from the primary acting transport of sodium. Secondary active reabsorption When you caught with sodium through a luminal membrane, the same way as glucose amino acids are reabsorbed, inorganic phosphate, sulfate and some organic nutrients. Low molecular weight proteins are reabsorbed by pinocytosis In the proximal segment. The protein reabsorption begins with endocytosis (pinocytosis) at luminal membrane. This energy-dependent process is initiated by the binding of the molecules of the profiltrated protein with specific receptors at the luminal membrane. Separate intracellular bubbles, which appeared during endocytosis, merge inside the cell with lysosomes, whose enzymes split proteins to low molecular weight fragments - dipeptides and amino acids, which are removed in the blood through the baselateral membrane. The separation of proteins with urine is not more than 20 - 75 mg per day, and with kidney disease, it may increase to 50 g per day (proteinuria ).
An increase in the separation of urine proteins (proteinuria) may be due to the impaired of their reabsorption or filtering.
Non-ionic diffusion - Weak organic acids and bases are poorly dissociated. Dissolve in the lipid matrix membranes and reabsorbed at a concentration gradient. The degree of their dissociation depends on the pH in the tubules: when it decreases dissociation acidic, rights increase. Acid reabsorption increases, basins - decrease. As an increase in the pH - on the contrary. This is used in the clinic to accelerate the removal of poisonous substances - in the poisoning of barbiturates, blood is larched. This increases their content in the urine.
Loop Genla. In the loop, Genla generally always reabsorb more sodium and chlorine (about 25% of the filtered number) than water (10% of the volume of filtered water). This is an important difference in the loop of Genla from the proximal tube, where water and sodium are reabsorbed almost in equal proportions. The descending part of the loop does not reabsorb sodium or chlorine, but it has a very high permeability for water and reabsorbing it. The ascending part (both thin and thick, its plot) recompensates sodium and chlorine and practically does not reabsorb water, because it is completely not permeable for it. The reabsorption of sodium chloride ascending part of the loop is responsible for the reabsorption of water in its descending part, i.e. The transition of sodium chloride from the ascending part of the loop in an interstitial liquid increases the osmolarity of this fluid, and this entails a greater reabsorption of water by diffusion from the water permeable descending part of the loop. Therefore, this section of the tube received the name of the distribution segment. As a result, the liquid is already a hyposotic in the ascending thick part of the loop of Genela (as a result of the sodium yield), it goes to the distal convulsion channel, where the breeding process continues and it becomes even more hyposotically, since in the subsequent areas of nephrone organic substances are not absorbed in them only ions are reabid and H 2 O. Thus, it can be argued that the distal convulsion canal and the ascending part of the loop of Genela function as segments where urine breeding occurs. As the collective tube of the brainstant is progressing, the tubular liquid becomes more and more hyperosmotic, because The reabsorption of sodium and water continues in the collecting tubes, in them the formation of finite urine (concentrated, due to the adjustable reabsorption of water and urea. H 2 O is translated into an interstitial substance according to the laws of osmosis, because there is a higher concentration of substances. reabsorption percentage Water can vary widely depending on the water balance of this body.
Distal reabsorption. Optional, adjustable.
Features:
1. The walls of the distal segment are badly permeable for water.
2. Here is actively rebupping sodium.
3. The permeability of the walls regulated : for water - antidiuretic hormone, for sodium - Aldosterone.
4. Indicates the process of secretion of inorganic substances.
The tubing reabsorption is the process of reverse absorption of water and substances from the urine-contained in the lumet in Limph and Blood.
The main mass of molecules is reabsorbed in the proximal department of nephron. Here are practically completely absorbed by amino acids, glucose, vitamins, proteins, microelements, a significant number of Na +, C1-, HCO3 ions and many other substances.
In the loop of Genela, the distal canal and collecting tubes are absorbed by electrolytes and water.
Aldosterone stimulates the reabsorption of Na + and the excretion of K + and H + to the renal tubules in the distal department of nephrone, in the distal canal and cortical collecting tubes.
Vasopressin promotes water reabsorption from the distal convolutions and collecting tubes.
With the help of passive transport, the reabsorption of water, chlorine, urea is carried out.
Active transport is called the transfer of substances against electrochemical and concentration gradients. Moreover, the primary-active and secondary-active transport are distinguished. Primary-active transport occurs with the cost of cell energy. An example is the transfer of Na + ions using the Na + / K + -at phase enzyme using ATP energy. With secondary-active transport, the transfer of the substance is carried out due to the energy of the transport of another substance. Glucose and amino acids are reabsorbed by the mechanism of secondary acts.
The magnitude of the maximum channel transport corresponds to the old concept of "renal threshold of removal". For glucose, this value is 10 mmol / l.
Substances, the reabsorption of which does not depend on their concentration in the blood plasma, are called non-negotiable. These include substances that are not reablied at all, (inulin, mannitol) or are very rebupported and stand out with urine in proportion to the accumulation of them in the blood (sulfates).
Normally, a small amount of protein falls into the filtrate and reabsorb. The process of protein reabsorption is carried out using pinocytosis. Entering the cage, the protein is subjected to hydrolysis from the enzymes of lysosomes and turns into amino acids. Not all proteins are subjected to hydrolysis, part of them goes into the blood unchanged. This process is active and requires energy. The appearance of protein in the urine is called proteinuria. Proteinuria can be in physiological conditions, an example, after severe muscular work. Basically, proteinuria takes place in pathology in jade, nephropathies, with myelomic disease.
The urea plays an important role in the mechanisms of concentration of urine, freely filtered in the gloms. In the proximal tubule, part of the urea is passively reabonbing due to the concentration gradient, which arises due to the concentration of urine. The rest of the urea comes to collecting tubes. In the collecting tubes under the influence of ADG, the reabsorption of water and the concentration of urea increases. ADG enhances the permeability of the wall and for urea, and it goes into the kidney cerebral, creating approximately 50% of osmotic pressure here. From the interstice at a concentration gradient urea diffuses in the loop of Genla and again enters the distal tubules and collective tubes. Thus, the intravenous urea cycle is performed. In the case of aqueous diurea, the absorption of water in the distal nephron stop is stopped, and urea is displayed more. Thus, its excretion depends on the diurea.
The reabsorption of weak acids and bases depends on what form they are in ionized or non-ionized. Weak bases and acids in ionized state are not reasurable and removed with urine. The degree of ionization of the base increases in an acidic medium, so they are excreted at a greater speed with sour urine, weak acids, by contrast, are faster with alkaline urine. It is of great importance, since many medicinal substances are weak bases or weak acids. Therefore, in poisoning with acetylsalicylic acid or phenobarbital (weak acids), it is necessary to introduce alkaline solutions (NaHCO3) in order to translate these acids into an ionized state, thereby contributing to their rapid excavation from the body. For rapid excretion of weak bottoms, it is necessary to introduce acidic products for acidification of urine into the blood.
Water is reabsorbated in all nephron departments passively due to the transport of osmotically active substances: glucose, amino acids, proteins, sodium ions, potassium, calcium, chlorine. When reabsorption of osmotically active substances decreases and reabsorption of water decreases. The presence of glucose in the final urine leads to an increase in diuresis (polyuria).
The main ion providing passive water absorption is sodium. Sodium, as mentioned above, is also required for glucose and amino acids. In addition, it plays an important role in creating a osmotically active medium in the interstation of the curse brain layer, due to which the urine concentration occurs.
The flow of sodium from the primary urine through the apical membrane inside the Channel epithelium cell occurs passively by electrochemical and concentration gradients. The excretion of sodium from the cell through basolateral membranes is actively using Na + / K + -atphase. Since the energy of cell metabolism is spent on the transfer of sodium, its transport is primary active. Sodium transport in the cell can occur due to different mechanisms. One of them is the exchange of Na + on H + (countercurrent transport, or antiport). In this case, sodium ion is transferred inside the cell, and the hydrogen ion is outward. Another path of sodium transfer to the cell is carried out with the participation of amino acids, glucose. This is the so-called kittensport, or sympathene. Partly sodium reabsorption is associated with the secretion of potassium.
Cardiac glycosides (Stroofantin K, Obaine) are able to coal the Na + / K + -ATPase enzyme, providing sodium transfer from the cell to the blood and transport of potassium from the blood to the cell.
Of great importance in the mechanisms of reabsorption of water and sodium ions, as well as the concentration of urine has the operation of the so-called rotary countercurrent multiplinary system. After passing the proximal segment of the channel, the isotonic filtrate in the reduced volume enters the loop of Genela. In this area, the intense reabsorption of sodium is not accompanied by reabsorption of water, since the walls of this segment are few permeable to water even under the influence of ADG. In this regard, the urine breeding occurs in the lumen of the nephron and the sodium concentration in the interstice. Divorced urine in the distal station of the tube loses excess fluid, becoming isotonic plasma. The reduced amount of isotonic urine enters the collecting system, in the brain layer, the high osmotic pressure in the interstation of which is due to the increased sodium concentration. In the collecting tubes, under the influence of ADG, the inverse absorption of water continues in accordance with the concentration gradient. The VASA RECTA passable in the brain layer is functioning as counter-case and metabolic vessels, taking off the path to sodium paresses and give it to a return to the cortical layer. In the depths of the brain layer, the high sodium content is maintained, providing resorption of water from a collective system and urine concentration.
The functions of the kidney channel apparatus (including proximal channels, nephron loop, distal channel and collective tubes) are:
- reabsorption of the part of the organic and inorganic substances profined in the clusher;
- secretion in the lumen of the tubular substances contained in the blood or the channels formed in the cells,
- Concentration of urine.
Reabsorption - This is the reverse absorption of various substances from the enlightenment of the tubules in the plasma of peritabular capillaries. Reabsorption occurs in all departments of the Netrone tubes, in a collecting tube and is determined by the characteristics of the structure of the channel epithelium of the kidneys. The surface of the cells of the proximal convulsion canal, converted into its lumen has a thick brushed glycocalix, which increases the area of \u200b\u200bthe membrane with the tubular liquid 40 times. Under the brush cut between the cells there are permeable dense connections.
Apical part of Plasmolamma Also called luminal, it has a high ion permeability, contains various carriers proteins and provides advantageously passive transport of various substances.
Basolateral part of the cell Increased by the folding membrane and contains a large number of mitochondria, which determines the concentration of active transport systems (ion pumps).
Threshold reabsorption Reflects the dependence of the suction of the substance from its concentration in the blood plasma. If the concentration of the substance in the plasma does not exceed a certain threshold level, this substance will be completely rebucing in the nephron tubules, if it exceeds it is not completely reabsorbing and appears in the final urine, which is associated with the maximum saturation of carriers.
Primary urine Passing through the tubules and cleaning tubes, before turning into the final urine, undergoes significant changes. The difference consists not only in its quantity (from 180 liters there remains 1-1.5 liters), but also quality. Some substances, the necessary organism, completely disappear from urine or becomes much less. Occurs reabsorption process. The concentration of other substances increases many times: they are concentrated when water reabsorption. Still other substances that were not at the primary urine
Appear in the final. This happens as a result of their secretion.
Reabsorption processes can be active or passive. For implementation active process It is necessary that there were specific transport systems and energy. Passive processes It is usually happening without energy costs according to the laws of physics and chemistry.
Canal reabsorption It happens in all departments, but its mechanism in different parts of non-etinakov. Conditionally you can highlight From departments: Proximal convulsion canal, nephron loop and distal crawl channel with a cleaning tube.
In the proximal convinced canal Amino acids, glucose, vitamins, proteins, microelements are completely reabsorbed. In the same department, about 2/3 of water and inorganic salts Na +, K + Ca2 +, Mg2 +, Cl-, NS07, i.e. Substances that need the body for its activities. The reabsorption mechanism is mainly directly or indirectly associated with Na + reabsorption.
Sodium reabsorption .
Most of Na + is reabsorbated against the concentration gradient due to ATP energy. Reabsorption Na + is carried out in 3 stages: The transfer of ion through the apical membrane of the epithelial cells of the tubules, transportation in the basal or lateral membrane and transfer through the indicated membranes into the intercellular fluid and into the blood. The main driving force of reabsorption is the transfer of Na + using Na +, K + -ATF-AZA through the basolateral membrane. It provides permanent ion outflows. As a result, Na + in a concentration gradient with the help of special formations of the endoplasmic reticulum enters the membranes returned in the intercellular medium. As a result of this constantly operating conveyor, the concentration of ions inside the cell and especially near the apical membrane becomes much lower than on the other side, this contributes to the passive admission of Na + into the cell on an ion gradient. In this way,
The 2 stages of the sodium reabsorption by the Channel cells are passive and only one, the final, requires energy costs. In addition, part Na + is reabsorbing passively in the intercellular intervals along with water.
Glucose. Glucose is reabsorbing along with Na + transport. In the apicial membrane cells there are special transporters. These are proteins with a molecular weight of 320,000, which in the initial sections of the proximal tube are transferred to each other Na + and one glucose molecule (a gradual decrease in glucose concentration in the urine leads to the fact that in the following region of the channel to transfer one glucose molecule already two Na +). The driving force of this process is also electrochemical gradient Na +. On the opposite side of the cell complex Na - glucose - the carrier decays to three elements. As a result, the carrier is released returns to its former place and again acquires the ability to transfer new Na + and glucose complexes. In the cell, the glucose concentration increases, due to which the concentration gradient is formed, which sends it to the basal-lateral membranes of the cell and provides an output to the intercellular fluid. From here glucose enters blood capillaries and returns to the overall blood flow. The apical membrane does not pass glucose back into the lumen of the Canalza. Transport porters glucose are contained only in the proximal secession of the tubules, so glucose is reabsorbing only here.
Fine In the usual level of glucose in the blood, and therefore the concentration of it in the primary urine, all glucose is rebucing. However, with an increase in blood glucose levels of more than 10 mmol / l (about 1.8 g / l), the power of transport systems becomes insufficient for reabsorption. The first traces of glucose nonreaczorbing In the final urine, it is detected when its concentration in the blood is exceeded. The higher the blood glucose concentration, the greater the amount of glucose nonreebsorbing. Before the concentration of its 3.5 g / l This increase is not yet directly proportionally, since the process does not turn on part of the conveyors. But, starting from the level of 3.5 g / lThe removal of glucose with urine becomes directly proportional to its concentration in the blood. In men The full load of the reabsorption system is observed when 2.08 mmol / min (375 mg / min) glucose, and in women - 1, 68 mmol / min (303 mg / min) at the rate of 1.73 m2 of the body surface.
Amino acids. The reabsorption of amino acids occurs in the same mechanism as the glucose reabsorption. Complete reabsorption of amino acids occurs already in the initial sections of the proximal tubules. This process is associated with the active reabsorption of Na + through the apical membrane of cells. Revealed 4 types of transport systems: a) for basic b) for acid c) for hydrophilic d) for hydrophobic amino acids. From the cells of amino acids passively in a gradient of concentrations pass through the basal membrane into the intercellular fluid, and from there - in blood. The appearance of amino acids in the urine may be a consequence of violation of transport systems or a very high concentration of it in the blood. In the latter case, the effect may appear, which by the mechanism resembles glucosuria - overloading transport systems. Sometimes there is a competitive acids of the same type for a common carrier.
Proteins. The reabsorption mechanism of proteins is significantly different from the reabsorption mechanism of the compounds described. Finding into the primary urine, a small amount of proteins is normal almost completely reabsorbated by pinocytosis. In the cytoplasm of cells of the proximal tubules, proteins decompose with the participation of lysosomal enzymes. Amino acids that are formed by the concentration gradient from the cell enter the intercellular fluid, and from there to the blood capillaries. In this way, it can reabsorvant to zo mg of protein per 1 min. In case of damage to the glomeruli in the filtrate, more proteins fall and part can flow in urine ( proteinuria).
Channel secretion.In modern physiological literature concerning the activities of the kidneys, the term secretion It has two values. Firstof these, it describes the process of transferring a substance through the cells from the blood in the lumen of the tubular in a constant form, which increases the speed of the excretion of the substance by the kidney. Second - Isolation from the cell into blood or in the lumen of the tube synthesized in the kidney of physiologically active substances (for example, prostaglandins, bradykin, etc.) or excreted substances (for example, hypuric acid).
Secretion of organic and inorganic substances - One of the important processes that ensure the process of urinations. Some fish in the kidney have lack of glitter. In such cases, secretion plays a leading role in the activities of the kidney. In the kidneys of most other classes of vertebrates, including in mammals, secretion provides the selection from the blood to the lumen of the tubules of additional quantities of some substances that can be filtered by the YB of kidney gloms.
In this way, secretion speeds up Highlighting by the kidney of some alien substances, finite exchange products, ions. In the kidney in mammals, organic acids are secreted (Penicillin, para-aminohypuric acid - Pag, diodewood, uric acid), organic bases (choline, guanidine), inorganic substances (potassium). The kidney glomerular and agglomelar sea bony fish is capable of secretion of magnesium ions, calcium, sulfates. There are places of secretion of different substances. In the kidney of all the vertebrates of the secretion of organic acids and bases, the cells of the proximal segment of the nephron, especially its direct part, the secretion of potassium mainly occurs in the cells of the distal convolve tube and collective tubes.
The mechanism of the secretion process of organic acids. Consider this process on the example of the highlighting of the kidney PAG. After introducing the PAG into the blood, its secretion by the kidney increases and the purification of blood from it significantly exceeds the amount of blood purification from the simultaneously entered inulin. This means that the pag is not only filtered in the glomers, but also in addition to the glomeruli in the lumen of the nephrone, there are significant quantities. It was experimentally shown that such a process was determined by the secretion of the PAG from the blood into the clearance of the proximal sections of the tubules. In the membrane cells of this tube facing the intercellular fluid, there is a carrier ( catransporter) High affinity for Pag. In the presence of the PAG, a complex of the carrier with a pag is formed, which moves into the membrane and on its inner surface is disintegrated, releasing the PAG into a cytoplasm, and the carrier acquires again the ability to move to the outer surface of the membrane and connect with the new PAG molecule. Mechanism of secretion Organic acids include a number of stages. In the basal plasma membrane, there is Na +, k + -atphase, which removes Na + ions from the cell and contributes to the ion intake to +. The lower concentration in the cytoplasm of Na + ions allows you to enter the Na + ion cells along the concentration gradient with the participation of sodium cooking. One of the types Such a cotrier contributes to the flow through the basal plasma membrane α-ketoglutarata and Na +. In the same membrane there is an anion exchanger, which removes α-ketoglutarate from the cytoplasm in exchange for a para-radium hydrochloric fluid coming from the intercellular fluid (PAG), diodewood or some other organic acids. This substance moves along the cell towards the luminal membrane and through it passes into the lumen of the station by the mechanism of lightweight diffusion.
Foreignness of breathing Cyanides, disagreement of respiration and oxidative phosphorylation by dinitrophenol reduces and stops secretion. In conventional physiological conditions, the level of secretion depends on the number of carriers in the membrane. The secretion of the PAG increases in proportion to the increase in the concentration of the PAG in the blood until all the carrier molecules are satisfied with the PAG. The maximum transport speed of the PAG is achieved at the moment when the amount of PAG available for transport is equal to the number of carrier molecules that can form a complex with a pagin. This value is defined as the maximum ability to transport the PAG - TRTR. The inclined PAG moves along the cytoplasm to the apical membrane and through it the special mechanism is released into the lumen of the Channel.
Ticket 15.
Previous3456789101112131415161718Next
Kidneys and their functions
Canal reabsorption
The initial stage of urica formation, leading to filtering of all low molecular weight components of blood plasma, inevitably must be combined with the existence in the kidney of systems, reabing all valuable substances for the body. Under normal conditions in the kidney of a person per day, up to 180 liters of filtrate is formed, and 1.0-1.5 l of urine is released, the remaining liquid is absorbed in the tubules. The role of cells of different nephron segments in reabsorption of non-etinakov. The experiments carried out on animals with the extraction of the micropipette of the liquid from different parts of the nephron made it possible to find out the peculiarities of the reabsorption of various substances in different parts of the renal tubules (Fig. 12.6). In the proximal nephron segment, amino acids, glucose, vitamins, proteins, microelements, a significant number of Na + ions, Ci-, NSOs are almost completely reabsorbed. In subsequent Nephron affairs are absorbed mainly electrolytes and water.
The reabsorption of sodium and chlorine is the most significant process in terms of volume and energy spent. In the proximal channel, as a result of the reabsorption of most of the profiled substances and water, the volume of primary urine decreases, and in the starting department of the nephron loop, about '/ s filmed in the glomerular to the liquid flows. Of the entire amount of sodium entered into the nephron when filtering, in the nephron loop absorbs up to 25%, in the distal sore tube - about 9%, and less than 1% is reabsorbing in collective tubes or excreted with urine.
Reabsorption in the distal segment is characterized by the fact that cells are transferred less than in the proximal channel, the number of ions, but against a larger concentration gradient. This nephron segment and collecting tubes play a crucial role in regulating the volume of urine released and the concentration of osmotically active substances (osmotic concentration1). Ultimate urine sodium concentration can decrease to 1 mmol / l compared to 140 mmol / l in blood plasma. In the distal tube, potassium is not only reabsorbing, but also secreted when it is excess in the body.
In the proximal department of nephrone, the reabsorption of sodium, potassium, chlorine and other substances occurs through a water-picered membrane of the canal wall. On the contrary, in the thick ascending area of \u200b\u200bthe loop of nephron, distal convolutions and collective tubes, the reabsorption of ions and water occurs through the water-permeable wall of the tube; The permeability of the water membrane in separate areas of nephron and collecting tubes can be adjusted, A.Veschina permeability varies depending on the functional state of the organism (optional reabsorption). Under the influence of pulses coming through the efferent nerves, and under the action of biologically active substances, the reabsorption of sodium and chlorine is regulated in the proximal department of nephrone. This is particularly clearly manifested in the event of an increase in blood volume and extracellular fluid, when a decrease in reabsorption in the proximal tube helps to increase the excretion of ions and water and thereby restoring water equilibrium. In the proximal canal is always preserved isosmia. The wall of the tubule is permeable for water, and the volume of reabsorbable water is determined by the amount of reabsorbed by osmotically active substances, which water moves along an osmotic gradient. In the finite parts of the distal nephron segment and collective tubes, the permeability of the water canal is regulated by vasopressin.
Optional water reabsorption depends on the osmotic permeability of the tubular wall, the magnitude of the osmotic gradient and the velocity of the fluid movement via the tube.
To characterize the absorption of various substances in the renal channels, an idea of \u200b\u200bthe elimination threshold is essential.
Non-profound substances are released at any concentration in blood plasma (and respectively in ultrafiltrate). These substances are inulin, mannitol. The threshold of the removal of almost all physiologically important, valuable substances for the body differ. So, the release of glucose with urine (glucosuria) occurs when its concentration in the glomerular filtrate (and in the blood plasma) exceeds 10 mmol / l. The physiological meaning of this phenomenon will be disclosed when describing the reabsorption mechanism.
Mechanisms of canalse reabsorption. Inverse absorption of various substances in the tubules is provided by active and passive transport. If the substance is reabidorized against electrochemical and concentration gradients, the process is called active transport. There are two types of active transport - primary-active and secondary-active. Primary-active transport is called in the case when the substance is transferred against an electrochemical gradient due to the energy of cell metabolism. An example is the transport of Na + ions, which occurs with the participation of the Na + enzyme, K + -at phase using ATP energy. The secondary-active is called the transfer of a substance against the concentration gradient, but without the energy costs of the cell directly to this process; So the glucose, amino acids are rehabitated. From the enlightenment of the station, these organic substances come into the cells of the proximal tubule using a special carrier, which must be attached to the Na + ion. This complex (carrier + organic substance + Na +) contributes to the movement of the substance through the brush cut membrane and its entry into the cell. The driving force of these substances through the apical plasma membrane is less than the concentration of sodium in the cytoplasm of the cell. The sodium concentration gradient is due to the unceasing active excavation of sodium from the cell into the extracellular fluid using Na +, K + -atphase, localized cells localized in lateral and basal membranes.
The reabsorption of water, chlorine and some other ions, urea is carried out with the help of passive transport - by electrochemical, concentration or osmotic gradient. An example of passive transport is reabsorption in the distal sore tube chlorine on an electrochemical gradient created by the active transport of sodium. On the osmotic gradient, water is transported, and the rate of its absorption depends on the osmotic permeability of the canal wall and the difference in the concentration of osmotically active substances on both sides of its wall. In the contents of the proximal tubule, due to the absorption of water and the substances dissolved in it, the concentration of urea is growing, a small amount of which at a concentration gradient is reabsorbing into blood.
Achievements in the field of molecular biology made it possible to establish the structure of molecules of ionic and water channels (aquaporins) receptors, outacoids and hormones and thereby penetrate the essence of some cellular mechanisms that provide transportation through the canal wall. Different properties of cells of different departments of nephron, unequal properties of the cytoplasmic membrane in the same cell. The apical membrane of the cell facing the lumen of the Canalza has other characteristics than its basal and side membranes are washed by the intercellular liquid and contact with the blood capillary. As a result, apical and basal plasma membranes participate in the transport of substances in different ways; The effect of biologically active substances on the other membrane is also specifically.
The cellular mechanism of reabsorption of ions Consider on the example Na +. In the proximal tube of nephrone, the absorption of Na + into the blood occurs as a result of a number of processes, one of which is active transport Na + from the enlightenment of the Canana, the other - the passive reabsorption of Na + after being actively transported into the blood of both hydrocarbonate ions and C1-. With the introduction of one microelectror in the lumen of the tubules, and the second - in the near-channel liquid, it was revealed that the potential difference between the outer and the inner surface of the proximal tube wall was very small - about 1.3 mV, in the area of \u200b\u200bthe distal tubule it can reach- 60 mV (rice .12.7). The lumen of both channels electronenered, and in the blood (consequently, in the extracellular fluid), the concentration of Na + is higher than in the liquid in the lumen of these tubules, so the reabsorption Na + is actively against the gradient of the electrochemical potential. In this case, from the lumen of the channel Na + enters the cell over the sodium channel or with the participation of the carrier. The inside of the cell is harnessed negatively, and positively charged Na + enters the cell according to the potential gradient, moves towards the basal plasma membrane, through which the sodium pump is thrown into the intercellular liquid; The potential gradient on this membrane reaches 70-90 mV.
There are substances that can affect individual elements of the Na + reabsorption system. Thus, the sodium channel in the membrane of the cell of the distal tubule and the collecting tube is blocked by amylorride and triamtenen, with the result that Na + cannot enter the channel. B cells there are several types of ion pumps.
Vanalis reabsorption and its regulation
One of them is Na +, K + -ATPase. This enzyme is in the basal and lateral cell membranes and provides transport Na + from the cell to the blood and flow from the blood to the K + cell. The enzyme is inhibited by cardiac glycosides, for example, Stulantin, Wabaine. In the reabsorption of the hydrocarbonate, an important role belongs to the carboanhydrase enzyme, the inhibitor of which is acetazolamide -one stops the reabsorption of the hydrocarbonate, which is excreted with urine.
The filtered glucose is almost completely reabsorbed by the cells of the proximal tube, and normally the amount (not more than 130 mg) is distinguished during the day (no more than 130 mg). The process of reverse absorption of glucose is carried out against a high concentration gradient and is secondaryly active. In the apical (luminal) membrane, glucose cells are connected to the carrier, which should also connect Na +, after which the complex is transported through the apical membrane, i.e., glucose and Na + are entered into the cytoplasm. The apical membrane is distinguished by high selectivity and one-sided permeability and does not let any glucose, nor Na + back from the cell in the lumen of the Channel. These substances move to the base of the cell according to the concentration gradient. The transfer of glucose from a cell to the blood through the basal plasma membrane is the character of light diffusion, A Na +, as already noted above, is removed by the sodium pump located in this membrane.
The amino acids are almost completely rebupported by cells of the proximal tube. There are at least 4 amino acid transport systems from the enlightenment of the Canana to the blood carrying out the reabsorption of neutral, bible, dicarboxylic amino acids and imino acids. Each of these systems provides suction of a number of amino acids of one group. Thus, the reabsorption system of bible amino acids is involved in the suction of lysine, arginine, ornithine and, possibly, cystine. When introduced into the blood, an excess one of these amino acids begins reinforced excretion of the amino acid kidney only this group. The transport systems of individual groups of amino acids are controlled by separate genetic mechanisms. Inheritance diseases described, one of the manifestations of which is the increased excretion of certain groups of amino acids (aminoaciduria).
Selection with urine of weak acids and bases depends on their glomerular filtration, reabsorption or secretion process. The process of deriving these substances is largely determined by the "non-ionic diffusion", the influence of which is particularly affected in the distal tubules and collecting tubes. Weak acids and bases may exist depending on the pH of the medium in two forms - non-ionized and ionized. Cell membranes are more permeable for non-ionized substances. Many weak acids with a greater speed are excreted with alkaline urine, and weak bases, on the contrary, with sour. The degree of ionization of the base increases in an acidic environment, but decreases in alkaline. In the non-ionized state, these substances through lipids are penetrated into the cells, and then in the blood plasma, i.e. they are reabsorbed. If the pH value of the canaly liquid is shifted into the acidic side, the base is ionized, poorly absorbed and excreted with urine. Nicotine is a weak base, at pH 8.1, 50% ionized, 3-4 times fasterly excreted with acidic (pH about 5) than with alkaline (pH 7,8) urine. The process of "non-ionic diffusion" affects the selection by the kidneys of weak bases and acids, barbiturates and other medicinal substances.
A small amount of protein profilt by the glomers is reabsorbed by cells of the proximal tubules. The selection of proteins with urine is not more than 20-75 mg per day, and with kidney diseases, it may increase to 50 g per day. An increase in the separation of proteins with urine (proteinuria) can be due to the impaired of their reabsorption or an increase in filtration.
Unlike the reabsorption of electrolytes, glucose and amino acids, which, penetrating through the apical membrane, is unchanged reached the basal plasma membrane and are transported in blood, the protein reabsorption is ensured by a fundamentally different mechanism. The protein enters the cage using pinocytosis. The filtered protein molecules are adsorbed on the surface of the apical membrane of the cell, while the membrane is involved in the formation of a pincite vacuole. This vacuum moves towards the basal part of the cell. In the near-choyondo region, where the plastic complex (Golgi apparatus) is localized, vacuoles can merge with lysosomes with high activity of a number of enzymes. In the lysosomes, the captured proteins are split and formed amino acids, dipeptides are removed into the blood through the basal plasma membrane. However, it should be emphasized that not all proteins are subjected to hydrolysis in the process of transport and part of them is transferred to the blood unchanged.
Definition of reabsorption in the kidney channels. Inverse absorption of substances, or in other words, their transport (T) from the enlightenment of the tubules into the tissue (intercellular) liquid and in blood, during reabsorption R (TRX) is determined by the difference between the amount of X (F ∙ PX ∙ FX), which filtered into Clushing, and the amount of substance allocated with urine (UX ∙ V).
TRX \u003d F ∙ PX.FX ─UX ∙ V,
where F is the volume of glomerular filtration, FX is a fraction of substance X, which is not associated with plasma proteins in relation to its overall concentration in the blood plasma, P is the concentration of the substance in the blood plasma, U is the concentration of the substance in the urine.
According to the above formula, the absolute amount of the reabsorbable substance is calculated. When calculating relative reabid-sorption (% r) determine the share of substance subjected to reverse absorption relative to the amount of substance profilt in the glomers:
% R \u003d (1 - EFX) ∙ 100.
To estimate the reabsorption capacity of the cells of the proximal tubules, the determination of the maximum magnitude of glucose transport (TMG) is important. This magnitude is measured in full saturation of the glucose system of its tubular transport (see Fig. 12.5). To do this, the glucose solution is poured into the blood and thereby increase its concentration in the glucopus filtrate until a significant amount of glucose begins to stand out with urine:
TMG \u003d F ∙ pg-ug ∙ V,
where f - glomeric filtering, pg is the glucose concentration in blood plasma, A Ug is the glucose concentration in the urine; TT - maximum channel transport of the studied substance. The value of TMG characterizes the full load of the glucose transport system; In men, this value is 375 mg / min, and in women - 303 mg / min at the calculation of 1.73 m2 surface of the body.
Canal reabsorption
The primary urine turns into a finite due to the processes that occur in the renal tubules and collective barrels. In the kidney of a person per day, 150 - 180 liters of the film, or the primary urine, is formed, and 1.0-1.5 l of urine is released. The remaining liquid is absorbed in the tubules and collecting tubes.
The tubing reabsorption is the process of reverse absorption of water and substances from the urine-contained in the lumet in Limph and Blood. The main meaning of reabsorption is to preserve the body all vital substances in the required quantities. Reverse absorption occurs in all nephron departments. The main mass of molecules is reabsorbed in the proximal department of nephron. Here are practically completely absorbed by amino acids, glucose, vitamins, proteins, microelements, a significant number of Na +, C1-, HCO3 ions and many other substances.
Scheme of canaly reabsorption
In the loop of Genela, the distal canal and collecting tubes are absorbed by electrolytes and water. Previously, it was believed that reabsorption in the proximal part of the canal was mandatory and unregulated. It is currently proved that it is regulated by both nervous and humoral factors.
Reverse absorption of various substances in the tubules can occur passively and actively. Passive transport occurs without energy costs for electrochemical, concentration or osmotic gradients. With the help of passive transport, the reabsorption of water, chlorine, urea is carried out.
Active transport is called the transfer of substances against electrochemical and concentration gradients. Moreover, the primary-active and secondary-active transport are distinguished. Primary-active transport occurs with the cost of cell energy. An example is the transfer of Na + ions using an enzyme Na +, K + - ATPase using ATP energy. With secondary-active transport, the transfer of the substance is carried out due to the energy of the transport of another substance. Glucose and amino acids are reabsorbed by the mechanism of secondary acts.
Glucose. It comes from the enlightenment of the Canalz to the cage of the proximal tube using a special carrier, which must be attached to the MA4 'ion. The movement of this complex inside the cell is carried out passively by electrochemical and concentration gradients for Na + ions. The low sodium concentration in the cell, creating a gradient of its concentration between the outer and intracellular medium, is ensured by the sodium-potassium membrane sodium-potassium pump.
In the cell, this complex decays into components. Inside the renal epithelium, a high concentration of glucose is created, therefore, in the further gradient, the concentration of glucose passes into an interstitial tissue. This process is carried out with the participation of the carrier due to the lightweight diffusion. Next, glucose goes into the bloodstream. Normally, with the usual concentration of glucose in the blood and, accordingly, all glucose is reabsorbed in the primary urine. With an excess of glucose in the blood, and therefore, in the primary urine, the maximum loading of channel transport systems can occur, i.e. All molecules-carriers.
In this case, glucose can no longer be reabidated and appears in the final urine (glucose). This situation is characterized by the concept of "maximum canal transport" (TM). The magnitude of the maximum channel transport corresponds to the old concept of "renal threshold of removal". For glucose, this value is 10 mmol / l.
Substances, the reabsorption of which does not depend on their concentration in the blood plasma, are called non-negotiable. These include substances that are not reablied at all, (inulin, mannitol) or are very rebupported and stand out with urine in proportion to the accumulation of them in the blood (sulfates).
Amino acids. The reabsorption of amino acids occurs also by the mechanism of associated with Na + transport. Amino acids filtered in the glomers are 90% reabsorbed by cells of the proximal kidney channel. This process is carried out using secondary-active transport, i.e. Energy goes to work sodium pump. At least 4 transport systems for the transfer of various amino acids (neutral, dioxide, dicarboxyl and amino acids) are distinguished. The same transport systems act in the intestine for absorption of amino acids.
Canal reabsorption
Genetic defects are described when certain amino acids are not reasurable and not absorbed in the intestine.
Protein. Normally, a small amount of protein falls into the filtrate and reabsorb. The process of protein reabsorption is carried out using pinocytosis. Epithelium of the renal tube actively captures the protein. Entering the cage, the protein is subjected to hydrolysis from the enzymes of lysosomes and turns into amino acids. Not all proteins are subjected to hydrolysis, part of them goes into the blood unchanged. This process is active and requires energy. During the day with the final urine, no more than 20-75 mg of protein goes. The appearance of protein in the urine is called proteinuria. Proteinuria can be in physiological conditions, an example, after severe muscular work. Basically, proteinuria takes place in pathology in jade, nephropathies, with myelomic disease.
Urea. It plays an important role in the mechanisms of urine concentration, freely filtered in the gloms. In the proximal tubule, part of the urea is passively reabonbing due to the concentration gradient, which arises due to the concentration of urine. The rest of the urea comes to collecting tubes. In the collecting tubes under the influence of ADG, the reabsorption of water and the concentration of urea increases. ADG enhances the permeability of the wall and for urea, and it goes into the kidney cerebral, creating approximately 50% of osmotic pressure here.
From the interstice at a concentration gradient urea diffuses in the loop of Genla and again enters the distal tubules and collective tubes. Thus, intravenous urea cycle is performed. In the case of aqueous diurea, the absorption of water in the distal nephron stop is stopped, and urea is displayed more. Thus, its excretion depends on the diurea.
Weak organic acids and bases. The reabsorption of weak acids and bases depends on what form they are in ionized or non-ionized. Weak bases and acids in ionized state are not reasurable and removed with urine. The degree of ionization of the base increases in an acidic medium, so they are excreted at a greater speed with sour urine, weak acids, by contrast, are faster with alkaline urine.
It is of great importance, since many medicinal substances are weak bases or weak acids. Therefore, in poisoning with acetylsalicylic acid or phenobarbital (weak acids), it is necessary to introduce alkaline solutions (NaHCO3) in order to translate these acids into an ionized state, thereby contributing to their rapid excavation from the body. For rapid excretion of weak bottoms, it is necessary to introduce acidic products for acidification of urine into the blood.
Water and electrolytes. Water is reabsorbated in all nephron departments. In the proximal convulsion canals, about 2/3 of all water is rebounded. About 15% is reabsorbated in the loop of Genla and 15% - in the distal convincing tubules and collective tubes. Water is reabsorbated passively due to the transport of osmotically active substances: glucose, amino acids, proteins, sodium ions, potassium, calcium, chlorine. When reabsorption of osmotically active substances decreases and reabsorption of water decreases. The presence of glucose in the final urine leads to an increase in diuresis (polyuria).
The main ion providing passive water absorption is sodium. Sodium, as mentioned above, is also required for glucose and amino acids. In addition, it plays an important role in creating a osmotically active medium in the interstation of the curse brain layer, due to which the urine concentration occurs. Sodium reabsorption is performed in all nephron departments. About 65% of sodium ions are reabsorbated in proximal tubules, 25% - in the nephron loop, 9% - in the distal sore canal and 1% - in collecting tubes.
The flow of sodium from the primary urine through the apical membrane inside the Channel epithelium cell occurs passively by electrochemical and concentration gradients. Sodium removal from the cell through basolateral membranes is actively using Na +, K + - ATPase. Since the energy of cell metabolism is spent on the transfer of sodium, its transport is primary active. Sodium transport in the cell can occur due to different mechanisms. One of them is the exchange of Na + on H + (countercurrent transport, or antiport). In this case, sodium ion is transferred inside the cell, and the hydrogen ion is outward.
Another path of sodium transfer to the cell is carried out with the participation of amino acids, glucose. This is the so-called kittensport, or sympathene. Partly sodium reabsorption is associated with the secretion of potassium.
Cardiac glycosides (stanfantine K, Obaine) are able to coal the Na + enzyme, K + - ATPase, providing sodium transfer from the cell to the blood and transport of potassium from the blood to the cell.
Of great importance in the mechanisms of reabsorption of water and sodium ions, as well as the concentration of urine has the operation of the so-called rotary countercurrent multiplinary system.
The swivel countercurrent system is represented by parallel with the knees of the loop of Genla and the collecting tube, along which the fluid moves in different directions (countermeasurely). The epithelium of the descending loop flows through water, and the epithelium of the rising knee is impenetrable for water, but is able to actively transfer sodium ions to the tissue fluid, and through it back to the blood. In the proximal department, the suction of sodium and water in equivalent quantities and urine here isotonic blood plasma.
In the downward department of the nephon loop, water is reabsorbed and urine becomes more concentrated (hypertensive). The return of water occurs passively due to the fact that in the ascending department at the same time the active reabsorption of sodium ions is carried out. Entering the tissue fluid, sodium ions increase the osmotic pressure in it, thereby contributing to the tissue liquid of water from the downward department. At the same time, an increase in the concentration of urine in the nefron loop due to the reabsorption of water facilitates sodium transition from urine into tissue fluid. Since in the ascending loop of the loop, the genle is reabsorbed by sodium, urine becomes hypotonic.
Following the collecting tubes, which are the third knee of the countercurrent system, urine can be strongly concentrated if an ADG acts that increases the permeability of water walls. In this case, as it moves along a collective tube into depth of the brainstant, more and more water goes into the interstitial fluid, the osmotic pressure of which is increased due to the content of large amounts of Na "1" and urea, and urine becomes increasingly concentrated.
When entering large amounts of water into the kidney body, on the contrary, large volumes of hypotonic urine are distinguished.
Channel reabsorption and secretion of substances in nephron.
Vanalis reabsorption or reverse absorption into the blood contained in the primary urine, water, salts, organic substances (glucose, protein, amino acids, vitamins).
The result is the reduction in the primary urine (by 70%), full reverse absorption into the blood for metabolism of substances (amino acids, glucose, many vitamins), partial absorption of water and ions Na, Cl, K, Ca, separation from blood to the urine of toxic metabolic products (urea, uric acid, ammonia, creatinine, sulfates, phosphates).
The absorption of basic substances is carried out using the mechanisms of active transport, diffusion and light diffusion.
For example:
The main ion that determines the osmotic pressure, and, consequently, the reabsorption of water, Na + enters the epithelial cells passively, according to the concentration gradient, and then discharged from the other side of the Na +-c-CAT-AZE cell.
Ions K + are reabsorbed actively on the apical membrane and then go into blood due to diffusion.
In the proximal convulsion canals, 70% of water and ions are rebounded.
The reabsorption of cations (Na +, K +, Ca2 +, Mg2 +) occurs against the concentration gradient, actively (using ATP energy).
Negatively charged anions are attracted by positively charged cations, and due to the electrostatic forces comes from urine into the blood passively (CL- and HCO3, following Na + and K +; SO42- and PO42- for CA2 + and MG2 +), water is succinn passively following ions on osmotic ions gradient.
The mechanisms of reabsorption Ca2 +, Mg2 +, SO4-, PO4 are similar to the reabsorption mechanisms Na +, K + and CL-.
Substances can be transferred to the cytoplasm of the renal epithelial cell by carriers in conjunction with Na + ions.
At the same time, from the epithelial cell in the blood, they come using diffusion across the concentration gradient.
At a certain concentration of blood substances (the deduction threshold), these substances (thresholds) will not be completely reabsorbed, and some of the profilt-contained substances will be in the final urine.
The thresholds include glucose, which is normal (4.6-7.2 mmol / l in blood) filtered, and then completely reabsorb.
With an increase in its concentration in the blood to 10.8 mmol / l, part of the glucose will not have time to reabsorb.
It stands out with urine from the body and glycosuria arises.
Reabsorption in various areas of neopinakov neodynakov.
In the proximal department, 40-45% of water, sodium, bicarbonates, chlorine, amino acids, glucose, vitamins, proteins, proteins, microelements by the end of the department remains 1/3 of the ultrafiltrate with the same osmotic pressure as in the plasma.
In the loop of Genela, 25-28% of water is reabsorbed, up to 25% sodium, as well as chlorine, potassium, calcium, magnesium ions
In the distal department - 10% of water, about 9% sodium, potassium.
In collecting tubes - 20% of water, less than 1% sodium.
The channel secretion is manifested by separation from the blood in the lumen of the channels of the products of the exchange and alien substances
The channel secretion is the result of active renal tubuine epithelium.
It is carried out against a concentration or electrochemical gradient and allows you to quickly excrete organic bases and ions, epithelial cells are secreted from choline blood, para -amicipuric acid, modified molecules of drugs and absorb glutamine from the primary urine.
With the help of the enzyme glutamine cleaved glutamine on glutamic acid and ammonia.
Ammonia is distinguished in the urine, which is made from the body in the form of ammonium salts.
In the same way, coal acid fermented carbonic acid is cleaved.
How is the process of reabsorption in the kidneys
Hs3 ions are absorbed into the blood (due to the electrostatic attraction of their Na + and K +).
H + ions are secreted in the urine, which is removed.
This explains the acidic reaction of finite urine (pH \u003d 4.5-6.5).
This mechanism prevents the body from the acidification.
Localization of secretion of substances in nephron is different
The jones of hydrogen and ammonia are secreted in the proximal department. And in the convoluted part, organic grounds are secreted:
Holine, Serotonin, Dopamine, Kinin, Morphine.
In the direct part - organic acids: para iaminogpurov, diodewood, penicillin, uric acid.
In the distal separator - para-amyptic acid, ammonia, H + and K + ions.
Medicinal substances are derived from the body using glomerular filtration (leftomycetin, streptomycin, tetracycline, neomycin, kanamycin, etc. Antibiotics).
With the help of the channel secretion, penicillin is derived (by 80-90%).
under the defeat of various departments of the nephron, a number of drug compounds are circulated in the blood and may not be released from the body.
In these cases, it is necessary to change the dosages of medicinal substances.







